Urachal Anomolies In Children
J. Christopher Austin, MD,
→ Enlace a la versión en español


Embryology and Anatomy
The urachus is a tubular structure that is patent during gestation. It connects the allantois at the umbilicus to the dome of the bladder during fetal development [1]. The lumen normally closes at about the twelfth week of gestation and obliterates completely. Following obliteration, all that typically remains is a fibrous cord running from the inferior aspect of the umbilicus to the dome of the bladder. The urachus is extraperitoneal and easily viewed during laparoscopic visualization of the pelvis (Figure 1).
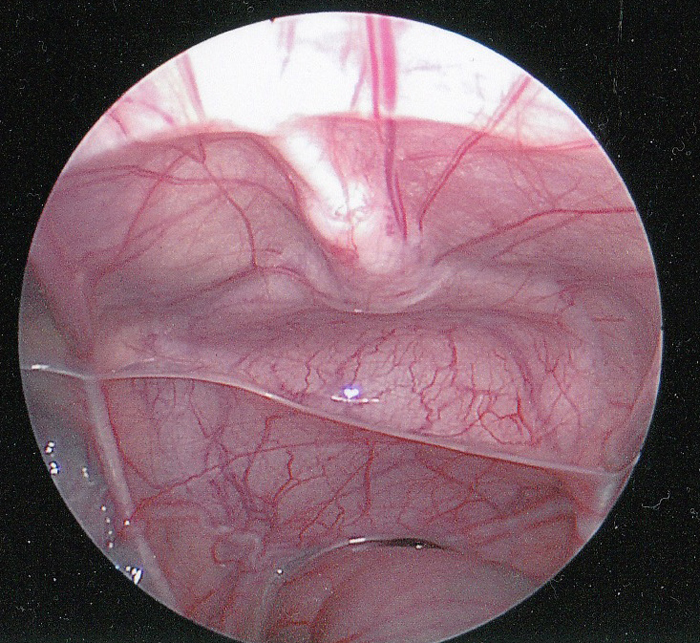
Figure 1- Intraperitoneal laparoscopic view of the urachus. The fibrous cord of the urachus (median umbilical ligament) is shown in the midline extending down to the dome of the bladder. The rectum is inferior. The vas deferens can be seen extending laterally just above the rectum.
The urachus is covered by the folds of peritoneum to form the median umbilical ligament. Rarely, the urachus may have gaps in the fibrous cord or even complete obliteration along its course from the umbilicus to the bladder dome. It is an important surgical landmark for marking the dome of the bladder to ensure proper placement of a vesicostomy and is removed en block with the bladder during radical cystectomy. There are conflicting opinions as to whether or not resection of the urachus for non-malignant conditions must include at least a small portion of the dome of the bladder [2-6]. In cases where there is doubt as to the whether the extent of the lesion includes the dome of the bladder it is prudent to include a small portion of the dome with the resection specimen. Most cases series report both techniques although the majority seem to favor including the dome of the bladder with no distinct difference in complications or outcomes.
The most common presenting symptoms in children with urachal anomalies are umbilical drainage or a mass and/or pain due to infection [3,4,6-10]. The umbilical drainage may be clear, serous, purulent, or bloody. Urachal abnormalities are a frequent concern in newborns with umbilical drainage that persists beyond a few weeks. Additionally, urachal anomalies may be incidentally discovered during radiographic examinations during the evaluation of children with urinary tract infections or hydronephrosis [7,8,10].
Classification of Urachal Anomalies
Urachal anomalies are due to failure of complete obliteration of the lumen during gestation [5]. Their anatomical classification is based on the degree to which the patency of the urachus has persisted. Typical urachal anomalies are shown in Figure 2. The possibilities vary from a completely patent urachus that allows urine to freely drain through the umbilicus to a small blind-ending sinus tract from the skin. A urachal cyst may be present at any location along the length of the urachus but are most commonly found near the dome of the bladder. A urachal diverticulum is a partial patency of the urachus draining into the dome of the bladder. The anomalies shown in Figure 2
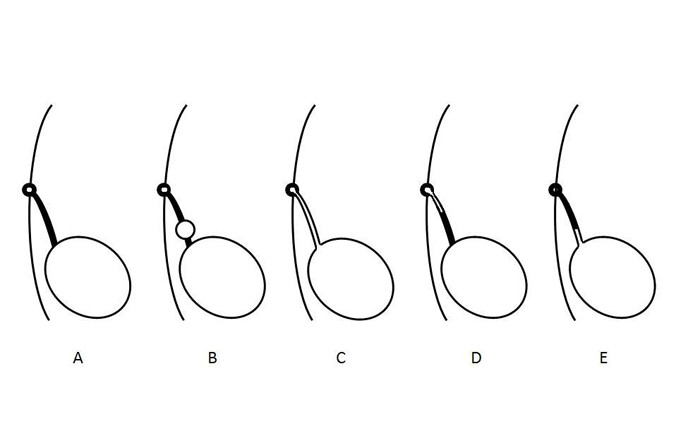
Figure 2- Diagram illustrating different types of urachal anomalies. A- Normal obliteration of the urachal lumen. B- Urachal cyst. C- Patent urachus. D- Urachal sinus. E- Urachal diverticulum.
are not exclusive as there can be combinations of the examples shown. For instance, there can be a urachal sinus associated with a urachal cyst. The relative incidence of the different types of urachal abnormalities from several clinical series are shown in Table 1.
Table 1- Summary of the Types and Incidence of Urachal Anomalies presenting in Children.
Author |
# Pts |
Patent |
Sinus |
Cyst |
Diverticulum |
Ashley |
46 |
6 |
14 |
25 |
1 |
Copp |
29 |
3 |
17 |
7 |
2 |
Cilento |
45 |
7 |
22 |
16 |
0 |
Galati |
23 |
2 |
9 |
12 |
0 |
Mesrobian |
21 |
2 |
9 |
9 |
1 |
Rich |
35 |
19 |
4 |
12 |
0 |
Yiee |
31 |
7 |
5 |
19 |
0 |
Total |
230 |
46 (20%) |
80 (35%) |
100 (43%) |
4 (2%) |
Urachal diverticulum seems to be the most rare of the anomalies in all series, with some recent series not reporting any [2-4,7-10]. Interestingly there is a single case report of a patent urachus that spontaneously closed with 2 weeks of catheter drainage and persisted as a urachal diverticulum [11]. Although only a single case, it suggests that there may be a dynamic evolution of the anomalies that may change over time if an infant is treated conservatively.
Clinical Presentation
Most childhood urachal remnants will present with either fluid drainage from the umbilicus or a mass with evidence of infection. There is a bimodal age distribution with presentation at a mean of 1-3 months of age for those with a urachal sinus or patency versus a mean age of 3 years for those who present with a urachal cyst [7]. The characteristics of the drainage fluid are a clue to its cause. Persistent clear fluid leakage (likely urine) in an infant is highly suggestive of a patent urachus while cloudy, serous, or bloody fluid is more indicative of an urachal sinus or cyst. The differential diagnosis of umbilical drainage also includes omphalitis, omphalomesenteric duct remnant, or an umbilical granuloma [4]. These non-urachal causes need to be considered during the evaluation of patients with umbilical drainage. The common presenting symptoms for urachal anomalies are shown in Table 2.
Table 2- Presenting Symptoms in Children with Urachal Anomalies.
Author |
# Pts |
Drainage |
Pain |
Mass/ |
Asymptomatic |
Other |
Cilento |
45 |
19 |
10 |
15 |
0 |
1 |
Copp |
29 |
13 |
0 |
10 |
5 |
1 |
Galati |
23 |
15 |
1 |
5 |
2 |
0 |
McCollum |
26 |
7 |
3 |
11 |
0 |
5 |
Mesrobian |
21 |
12 |
4 |
4 |
0 |
1 |
Yiee |
37 |
20 |
4 |
8 |
2 |
3 |
Total |
181 |
86 (48%) |
22 (12%) |
53 (29%) |
9 (5%) |
11 (6%) |
Physical examination may also be helpful. A patent urachus or urachal sinus can appear as a dimple or indentation in the base of the umbilicus (Figure 3).
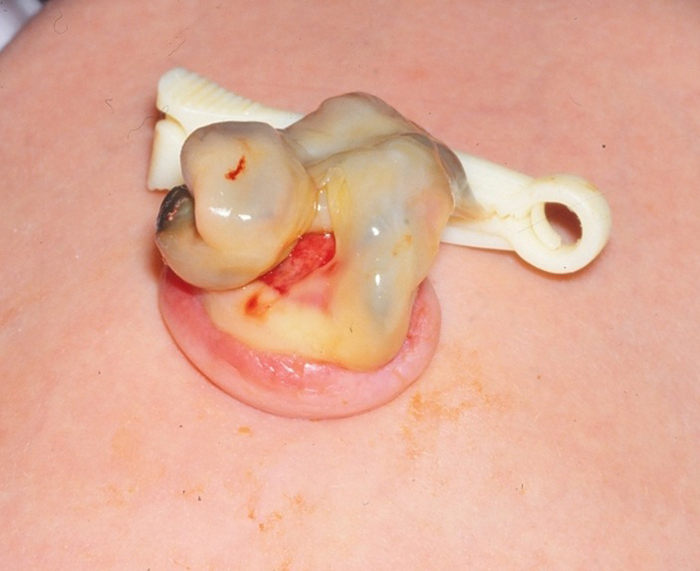

Figure 3- Patent urachus in a newborn. 3a- Demonstrates the beefy red appearance of the umbilical end of a patent urachus. 3b- The umbilical skin has been everted and a small feeding has been passed through the patent urachus into the bladder.
Some urachal anomalies are incidentally discovered during the routing radiographic evaluation of other disorders, such as urinary tract infections or prenatal hydronephrosis. Urachal cysts are likely to be seen during ultrasound imaging of the bladder (Figure 4).
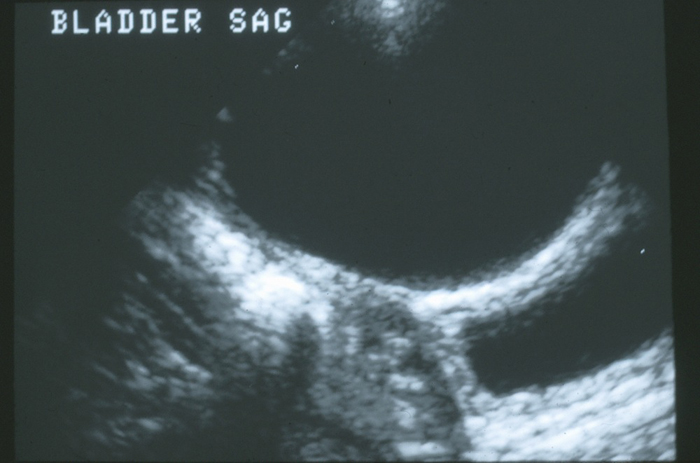
Figure 4- Sagittal view if the dome of the bladder in the midline. There is a large anechoic urachal cyst anterior to the bladder wall.
Urachal Carcinoma
As urachal carcinoma is not a disease reported to present in children or adolescents, the treatment of this disorder will not be included in this chapter [9,12]. As will be discussed in the section on management is it unknown what the risk is an asymptomatic urachal anomaly will go on to develop carcinoma and thus the value of prophylactic excision of an asymptomatic urachal anomaly is of unknown value. The most worrisome findings in a urachal anomaly for carcinoma is size greater than 4 cm and age greater than 55 years. Calcifications are a feature that is more common in carcinoma [9,12]. Whether calcifications in an asymptomatic benign urachal remnant is a predisposition to develop carcinoma is unknown, but it would seem prudent to remove lesions with calcifications, given that calcifications that may be associated with chronic inflammation, which is associated with carcinogenesis.
Radiologic Evaluation
Imaging is directed by the presenting symptoms and the degree of clinical suspicion [4,7]. A patent urachus that allows urine to drain freely through the umbilicus can be imaged with a high degree of sensitivity with either a voiding cystourethrogram (VCUG) or sinogram. The author prefers to evaluate children with a VCUG as it will not only identify the patent urachus, but also provide an anatomical assessment of the bladder, evaluate for bladder outlet obstruction, and the presence of vesicoureteral reflux (Figure 5).
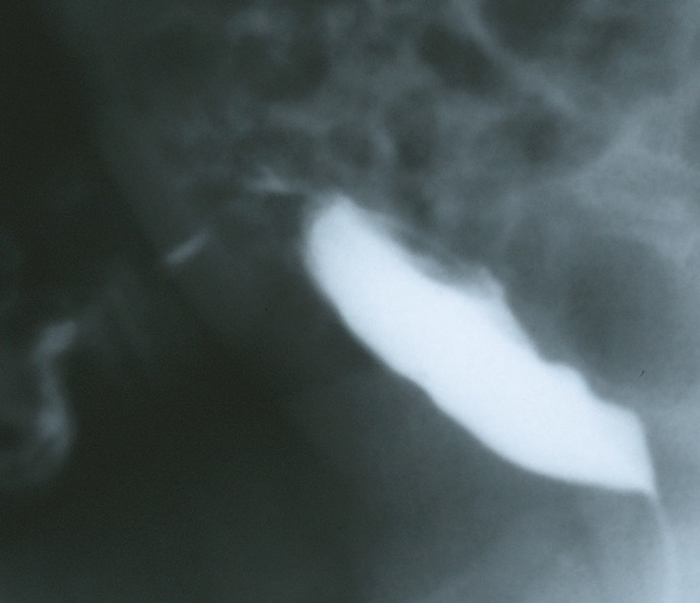
Figure 5- Lateral filling view from a VCUG in an infant with copious amounts of clear fluid draining from the umbilicus. The image demonstrates contrast draining through the anterior abdominal wall from the dome of the bladder via the patent urachus.
Although the chance of finding other associated anomalies of the genitourinary tract is low in patients with a patent urachus, the evaluation should also include a renal ultrasound to ensure the absence of hydronephrosis or other congenital kidney anomalies [4,7,10,13]. The incidence of concomitant kidney abnormalities has varied widely in published series, but given the lack of morbidity and risk with ultrasound, it is prudent to include imaging the kidneys as part of the work-up.
A urachal cyst greater in size than a few millimeters can be readily imaged by ultrasound. They may be incidentally detected in asymptomatic children when the bladder is examined during routine ultrasonographic evaluation, such as after a urinary tract infection. If there is any significant distance from the bladder the cyst may not be easily seen, and thus it is important to notify the ultrasonographer of the clinical suspicions when following or evaluating a possible urachal anomaly so that midline abdominal wall can be thoroughly examined in addition to the dome of the bladder. Infected urachal cysts appear as large heterogenous masses with complex fluid collections (Figure 6).
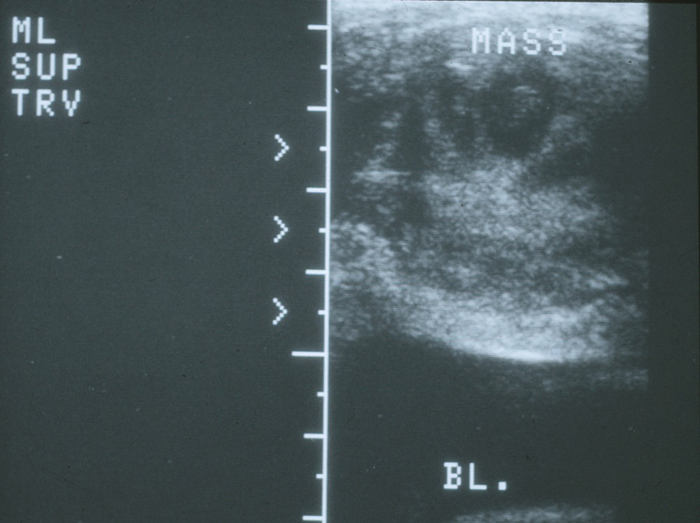
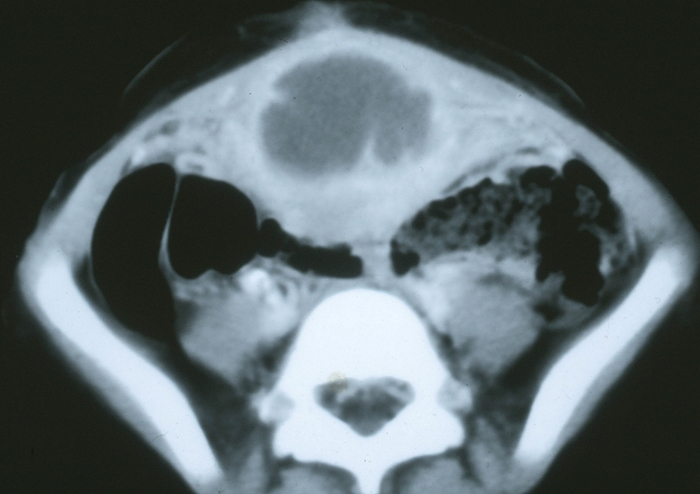
Figure 6- Infected urachal cyst. 6a- Transverse view of the bladder dome in the midline demonstrating a heterogeneous echogenic mass above the bladder. 6b- CT scan showing the midline mass with central fluid density consistent with an abscess and inflammatory stranding of the adjacent anterior abdominal wall.
The lesions may be several centimeters in diameter and can, on occasion, spread beyond the pre-peritoneal space and perforate the peritoneal cavity [14,15]. In cases where there is diagnoses is uncertain, a computed tomography scan (CT) can give excellent anatomical detail (Figure 7).
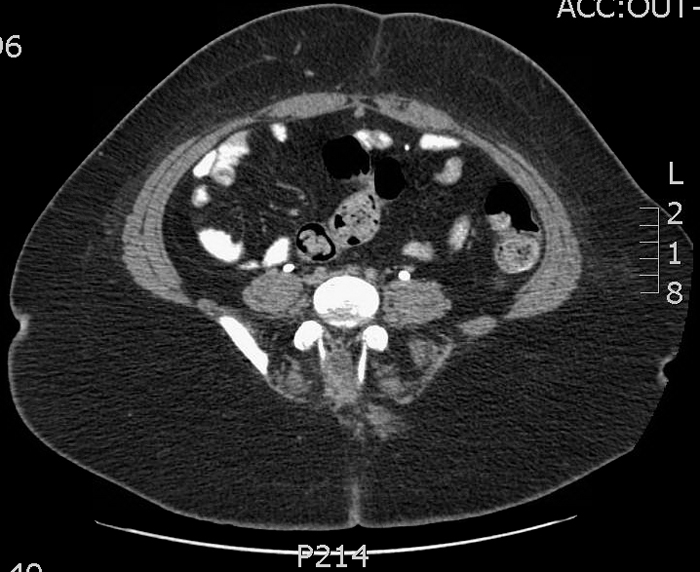
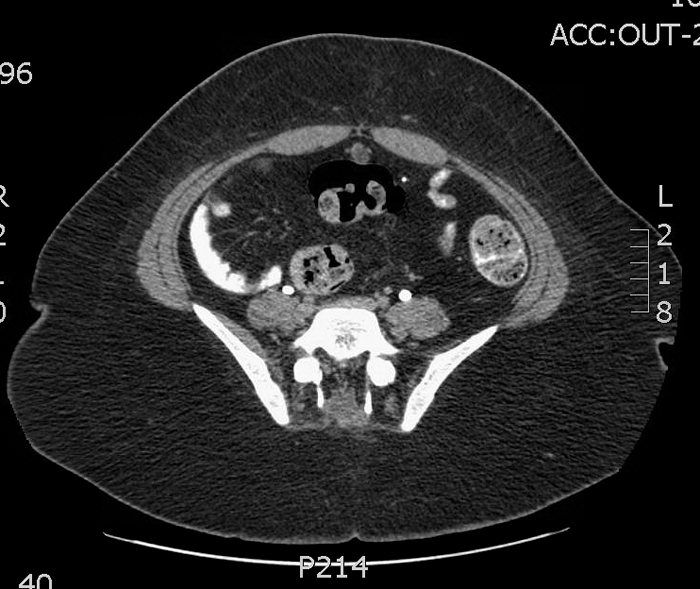
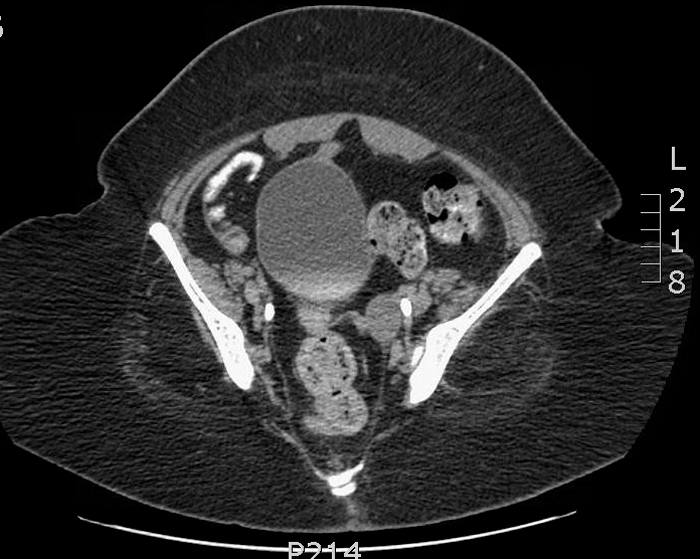
Figure 7- CT scan in a patient with recurrent bloody umbilical drainage. 3a- Image just inferior to the umbilicus demonstrate a normal appearing urachus (fibrous cord) just inferior to the rectus muscles in the midline. 3b- A urachal cyst is demonstrated more inferiorly. 3c- The proximity of the inferior extent of the cyst and the dome of the bladder is demonstrated.
Given the current practice to minimize radiation exposure in children to a level as low as possible, CT should not be considered an integral component of the routine workup. However, in cases where there is a high degree of clinical suspicion with a negative ultrasound (such as recurrent bloody umbilical drainage), a CT can be helpful in imaging the urachus and showing lesions which may be missed by ultrasound.
Treatment
In general, symptomatic urachal remnants should be treated with surgical excision. This should include complete excision of the urachus from the umbilicus to the dome of the bladder (Figure 8).
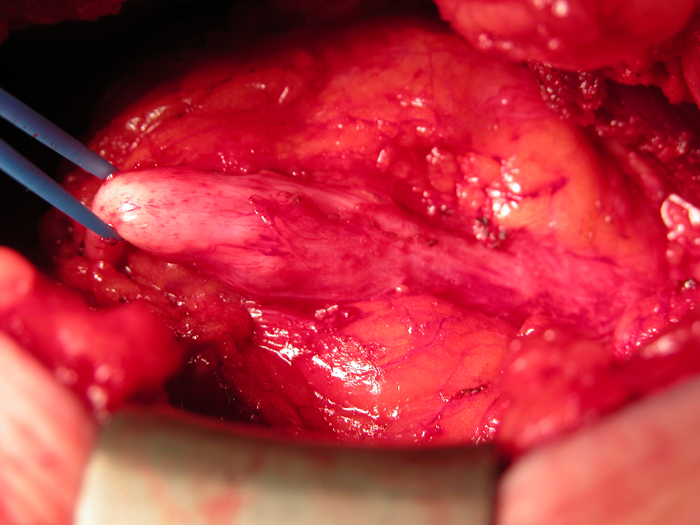

Figure 8- - Open excision of urachal cyst. 8a- Intra-operative view of a urachal cyst excision via an infra-umbilical midline incision. The cyst is in center with the bladder attachment to the right, and the fibrous cord extending to the umbilicus on the left. 8b- The specimen (cyst) after excision with the small cuff of bladder (right end of specimen).
There is controversy over whether the dome of the bladder must be included, as the fibrous cord or cyst may be able to be excised without entry into the bladder (not a possibility with a patent urachus however, which must be completely excised) [2-6]. Infected urachal cysts present another dilemma, as the marked enlargement of the cyst due to infection and surrounding inflammation make simple excision more difficult and may increase the risk of complications. One can approach the infected urachal cyst in either a single or staged approach [2,3,16-18]. The relative merits and risks of the two approaches will be further discussed below.
Surgical excision of the urachal remnant is curative and there are no functional sequelae from its excision, as it is a vestigial remnant. The main surgical dilemma occurs in patients who present with an asymptomatic lesion that is incidentally discovered in imaging. Pathological analysis of excised urachal remnants showed persistent epithelium in the remnant [10]. Multiple histologic types can be present including transitional, squamous, metaplastic , and gastrointestinal. Transitional is the most common. The presence of gastroinstestinal mucosa is a rare finding. There was no epithelium present in only a minority of samples and it was distributed along the various types of remnants. Thus the type of urachal anomaly was not predictive of the presence or absence of luminal epithelium. Whether the lesion was symptomatic or asymptomatic was not predictive either. Thus all types of urachal anomalies are at risk of containing non-regressed epithelium. The malignant potential of persistent epithelium in the urachus is unknown but is a concern. This finding favors the excision of remnants due to the potential future risk of tumor formation.
Conservative Management
For a surgeon it can be a more difficult decision not to operate. This is true for asymptomatic urachal anomalies. Children have a long life expectancy and the lack of reliable information about the long-term risk of infection or malignancy, which are the two most significant long-term morbidities of urachal anomalies, is of concern when deciding to follow a conservative approach. The most common lesion that is incidentally found is a urachal cyst [7,8]. The age of the patient, risk of anesthesia from any co-morbid conditions, and the circumstances under which the cyst was discovered need to be considered. If the patient is being evaluated for urinary tract infection and found to have vesicoureteral reflux, it may be prudent to wait until one has decided whether the reflux will need surgical correction, as the urachal cyst can easily be excised during ureteral reimplantation surgery. Recent publications have argued for a conservative approach [8,11]. There have been documented reports of spontaneous closure of patent urachuses and spontaneous regression of urachal cysts in children under 6 months of age. This argues for all children under the age of 6 months with an asymptomatic urachal abnormality to be initially managed with a conservative approach, with surgical excision reserved for those in whom the lesions persist as they are followed over the next 6-12 months. No morbidities have been reported with short-term observation for clinical or radiological follow-up, but most patients in these series were followed for less than 1 year. If one does take a conservative approach, it is important to educate the parents on the signs and symptoms of an infected urachus, as well as warn them that once the urachal remnant becomes infected, a simple outpatient excision then becomes a more complicated, possibly even staged, procedure.
Management of Infected Urachal Cysts
The initial management should focus on controlling the infection. To help direct antibiotic therapy, urine culture and culture of any wound drainage, if present, should be obtained. If the patient is febrile blood cultures should be obtained. Broad spectrum antibiotics should be started. The most common organism cultured from infected urachal cysts is Staphalococcus aureus (Table 3)
[6,8Table 3- Microbial Species cultured from Infected Urachal Remnants.
Author |
# Pts |
S. Aureus |
Strep sp |
Other * |
Ashley |
9 |
6 |
1 |
2 |
Galati |
5 |
5 |
0 |
0 |
McCollum |
9 |
6 |
1 |
2 |
Minevich |
9 |
9 |
0 |
0 |
Newman |
5 |
3 |
0 |
2 |
Total |
37 |
29 (79%) |
2 (5%) |
6 (16%) |
*E Coli-3, Citrobacter, Enterococcus, and Proteus.
,9,16,17]. Antibiotics should be chosen with the local resistance patterns of those organisms in mind. If the patient is stable, afebrile, non-toxic, without peritoneal signs, spreading cellulitis, or signs of fasciitis, initial management with antibiotics alone can be considered.
There are differing approaches to the surgical treatment of the infected urachal cyst. It essentially comes down to initial complete surgical excision vs. drainage (or initial therapy with antibiotics only) and delayed excision after the initial inflammatory response of the acute infection has subsided. The author’s treatment of choice has typically been the staged approach. It has been long-standing surgical dogma that it is of paramount importance that the urachus needs to be removed, not just drained, to prevent recurrent infection.
In the single-stage excision of the infected urachus, the margins of resection will be larger and result in larger soft tissue defect and the extent of the inflammation can extend intraperitonealy, which puts the abdominal viscera at risk. There is a small but significant risk of an enterocutaneous fistula and a higher rate of wound complications after primary excision of an infected urachal cyst compared to a staged approached [6,16,18].
In the staged approach, if the child is highly symptomatic or not responding to antibiotic therapy alone, the abscess can be drained either percutaneously or via an open incision. Neither is perfect, as the percutaneous drain (which can be placed with either ultrasound or CT guidance) may incompletely drain a multiloculated fluid collection. A percutaneously placed pigtail drain will help guide the secondary resection of the cyst wall during the second procedure. If no drain is left it is often difficult to identify the cyst wall in the fibrotic scar tissue that remains after the initial drainage during exploration at the second stage. Open drainage can more effectively drain loculated fluid collections, but unless a drain is left through the incision, it will again be difficult to identify the cyst walls after the inflammation has subsided. After the inflammation has subsided, the mass will no longer be enlarged (most infected urachal cysts appear very large [3-6 cm] when infected) and the cyst’s wall can be difficult to localize within the local tissue fibrosis and scarring secondary to the infection and prior surgery. There is controversy as to whether additional surgery after the initial incision and drainage is necessary, but it seems prudent to attempt complete resection of the urachus after a significant infection.
Laparoscopic Excision of the Urachus
In this era of minimally invasive surgery, multiple reports of laparoscopic, and more recently, robotic-assisted laparoscopic resection of urachal remnants in children have emerged [19-21]. Laparoscopic single site surgery has been reported as well [22]. The main advantage of robotic technology is during closure of the dome of the bladder for surgeons who aren’t as adept with their laparoscopic suturing skills [21]. Visualization is excellent with a laparoscopic approach for the bladder but can be more challenging at the umbilicus if the ports are not carefully placed. The urachus should be resected from the base of the umbilicus to the dome of the bladder. Again, there is controversy as to whether or not complete resection requires excision of the dome of the bladder [19,20]. If there is any doubt as to the extent of the lesion being excised, then one should err on the side of a more complete resection. Port placement is an important consideration [20]. Since the urachus originates at the umbilicus, this cannot be used as a port site. The most common site for the camera is supra-umbilical (usually 1-2 cm). This gives enough working space to visualize the dissection from the umbilicus to the dome of the bladder. Working ports should be placed laterally on either side, usually at the level of the umbilicus. They need to be lateral enough to give the mobility needed to start the dissection up at the umbilicus. Alternatively, lateral working ports and camera placement (on either the right or left side of the abdomen) offers lateral visualization of the urachus and keeps all the ports infra-umbilical in location. The lateral port configuration will make suturing the bladder closure more difficult due to the angle. Techniques advocated for the closure of the bladder dome or the urachal attachment to the bladder have included the use of the GIA stapler, direct suturing with absorbable suture, and clips. Although there are no reports of stones forming at the dome of the bladder associated with staples, it would seem prudent to use a closure technique that doesn’t leave permanent metallic clips or staples in the bladder wall.
Open Excision of the Urachus
In infants and small children complete resection of the urachus can easily be accomplished through a small incision. It can be oriented in either a transverse or vertical midline. For infants, a small 1-1.5 cm incision midway between the pubis and umbilicus will give access to the urachus and allow complete resection from the umbilicus to the dome of the bladder with excellent exposure of bladder dome for closure. This small incision is comparable to the size of incision needed for the 12 mm camera port of the surgical robot and keeps the procedure entirely extra-peritoneal, eliminating potential intra-abdominal complications. In older or obese children or adolescents, it is prudent to make a vertical midline incision. If there is trouble with exposure, the incision can be extended up toward the umbilicus or down toward the bladder to facilitate complete removal of the urachus in these patients. Complications rates for simple excision are very low and the surgery can either be performed as an outpatient or with a short hospital stay if a catheter is left in place. Urine leaks or wound complications are more commonly associated with single-stage excision of infected cysts and not simple excision [6,16].
Summary
Urachal anomalies may present in various forms. They typically present with umbilical drainage or infection (suprapubic mass). Asymptomatic anomalies may be found on ultrasound or VCUG studies evaluating children for urinary tract infections. Symptomatic urachal anomalies should be surgically excised. There is controversy as to whether or not asymptomatic anomalies need treatment. Histological studies show that most urachal anomalies have some persistent epithelium. The true risk of infection or malignant degeneration for these is not known. Simple excision should prevent these conditions from developing, and given the relatively benign nature of excision versus treating an infected anomaly and the usual advanced stage of urachal carcinoma at presentation and poor prognosis, early treatment seems a logical choice.
References
References
Patrzyk M, Glitsch A, Schreiber A, von Berstorff W, Heidecke CD. Single-incision laparscopic surgery as an option for the laparoscopic resection of an urachal fistula: first description of the surgical technique. Surg Endosc 2010: 24:2339-2342.

 |
 |
 |
 |
 |
 |
 |
 |